Primum non nocere. The first principal of medicine. First do no harm. In other words, as a doctor, you may or may not be able to help your patient, but at the very least, don’t make things worse.
This is the over-arching principal that is taught from day one medical school. This principal along with ever looming shadow of litigation tends to make medics cautious about offering treatments. Wait for the innovators and early adopters to do the spade work. See how things pan out. If the treatment and published data seem promising, then go to the courses, learn the techniques and add the treatment to your list. Another string to your bow.
This is the usual way for medicine to advance and techniques to develop. However, this ideal broke down in 3 particular areas of medicine to the point that the then Secretary of State for Health, Jeremy Hunt, in 2018 ordered an public enquiry. The Independent Medicines and Medical Devices Safety Review was commissioned to examine the practice of pelvic mesh implants for the treatment of vaginal prolapse and stress incontinence. It also examined the practice of Primidos – a hormonal pregnancy detector used from the 1950’s to 1978 and the prescription practices of sodium valproate, an anti-epileptic drug, known to harm unborn babies, during pregnancy.
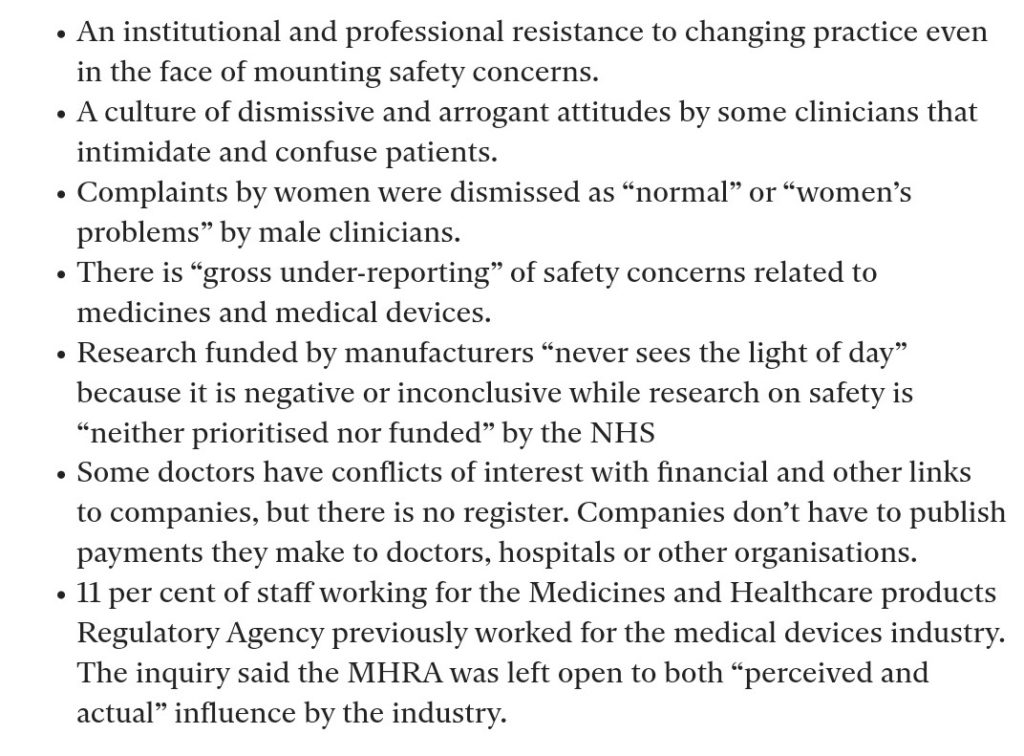
This enquiry, chaired by Baroness Julia Cumberlege, was published on 8th July 2020 and was a damning critique of practice in these areas. It makes for uncomfortable reading for any medic.
Cumberlege made 9 recommendations as a result of her inquiry. These were as follows:-
Recommendation 1: The Government should immediately issue a fulsome apology on behalf of the healthcare system to the families affected by Primodos, sodium valproate and pelvic mesh.
Recommendation 2: The appointment of a Patient Safety Commissioner who would be an independent public leader with a statutory responsibility. The Commissioner would champion the value of listening to patients and promoting users’ perspectives in seeking improvements to patient safety around the use of medicines and medical devices.
Recommendation 3: A new independent Redress Agency for those harmed by medicines and medical devices should be created based on models operating effectively in other countries. The Redress Agency will administer decisions using a non-adversarial process with determinations based on avoidable harm looking at systemic failings, rather than blaming individuals.
Recommendation 4: Separate schemes should be set up for each intervention – HPTs, valproate and pelvic mesh – to meet the cost of providing additional care and support to those who have experienced avoidable harm and are eligible to claim.
Recommendation 5: Networks of specialist centres should be set up to provide comprehensive treatment, care and advice for those affected by implanted mesh; and separately for those adversely affected by medications taken during pregnancy.
Recommendation 6: The Medicines and Healthcare products Regulatory Agency (MHRA) needs substantial revision particularly in relation to adverse event reporting and medical device regulation. It needs to ensure that it engages more with patients and their outcomes. It needs to raise awareness of its public protection roles and to ensure that patients have an integral role in its work.
Recommendation 7: A central patient-identifiable database should be created by collecting key details of the implantation of all devices at the time of the operation. This can then be linked to specifically created registers to research and audit the outcomes both in terms of the device safety and patient reported outcomes measures.
Recommendation 8: Transparency of payments made to clinicians needs to improve. The register of the General Medical Council (GMC) should be expanded to include a list of financial and non-pecuniary interests for all doctors, as well as doctors’ particular clinical interests and their recognised and accredited specialisms. In addition, there should be mandatory reporting for the pharmaceutical and medical device industries of payments made to teaching hospitals, research institutions and individual clinicians.
Recommendation 9: The Government should immediately set up a task force to implement this Review’s recommendations. Its first task should be to set out a timeline for their implementation.